ERP for Healthcare in 2026: The Complete Guide to Finance and AI Automation
A practical guide to healthcare ERP systems, key finance challenges, and how AI automation improves invoice matching, procurement, and audit readiness.
If you work in healthcare finance, you have felt this before. Invoices stuck in approval queues. Purchase orders that take days. A month-end close that bleeds into the following week. An audit request that triggers a three-day document hunt.
This guide is for CFOs evaluating a new system, finance directors fixing what is broken, operations leaders trying to understand why procurement is slow, and anyone newer to the industry who wants to understand how healthcare finance actually works. No technical background needed. By the end, you will know what to look for, what to avoid, and what good looks like.
What Is an ERP, and Why Does It Matter?
ERP stands for Enterprise Resource Planning. The idea is simple: one system that connects all the financial and operational work of a business, connecting purchasing, payments, budgets, and reporting, so everything is in one place instead of scattered across spreadsheets, email threads, and separate tools.
Think of it as the financial nervous system of an organization. Every time someone buys something, pays a vendor, or closes the books, the ERP is involved.
For most businesses, a good ERP means cleaner books and less manual work. For healthcare organizations, the stakes are higher. Hundreds of vendors, complex purchasing rules, regulatory audits, and tight budgets, often all at the same time.
How Healthcare Finance Is Different from Every Other Industry
A retailer buys products and sells them. A manufacturer processes raw materials. Both have relatively straightforward financial flows.
A hospital is different. You are buying surgical supplies, pharmaceuticals, facility services, and IT equipment, each with different pricing rules, delivery requirements, and compliance obligations. Some purchases are tied to national group contracts. Some items carry expiry dates and lot numbers that must be tracked. Some vendors must be screened against federal exclusion lists before you can pay them.
Revenue does not arrive cleanly either. Insurers pay weeks or months after services are delivered, at rates that may differ from what was billed. Grant-funded programs require separate accounting. Every transaction has to be documented in case an auditor asks.
Generic business software handles some of this. The parts it cannot handle become manual workarounds, and those workarounds quietly cost money and create risk every day.
What an ERP Actually Does in a Hospital or Health System
An ERP in healthcare is not a clinical system. It does not touch patient records. It manages everything that supports care delivery from the business side, across four core areas.
Procurement. A clinical department raises a need. The ERP checks the budget, confirms the contracted price, routes the request for approval, and dispatches a purchase order. Without this in one system, purchasing becomes fragmented and uncontrolled.
Accounts Payable. When the vendor's invoice arrives, someone verifies it matches what was ordered and received, codes it to the right cost center, gets it approved, and schedules payment. A 500-bed hospital does this thousands of times a month. Understanding the full accounts payable workflow is essential before choosing any ERP platform.
General Ledger and Reporting. Every transaction flows into the financial accounts. The ERP produces the reports the CFO, the board, and auditors rely on.
Budgeting and Cost Tracking. Departments receive budget allocations. The ERP tracks spending in real time and flags when limits are being approached.
When these four functions work together, finance teams have visibility and control. When they are handled by separate tools, gaps appear, and gaps in healthcare finance become audit findings.
How a Healthcare Invoice Moves Through the System
Most people outside finance do not realize how many steps sit between a clinical department raising a need and a vendor getting paid.
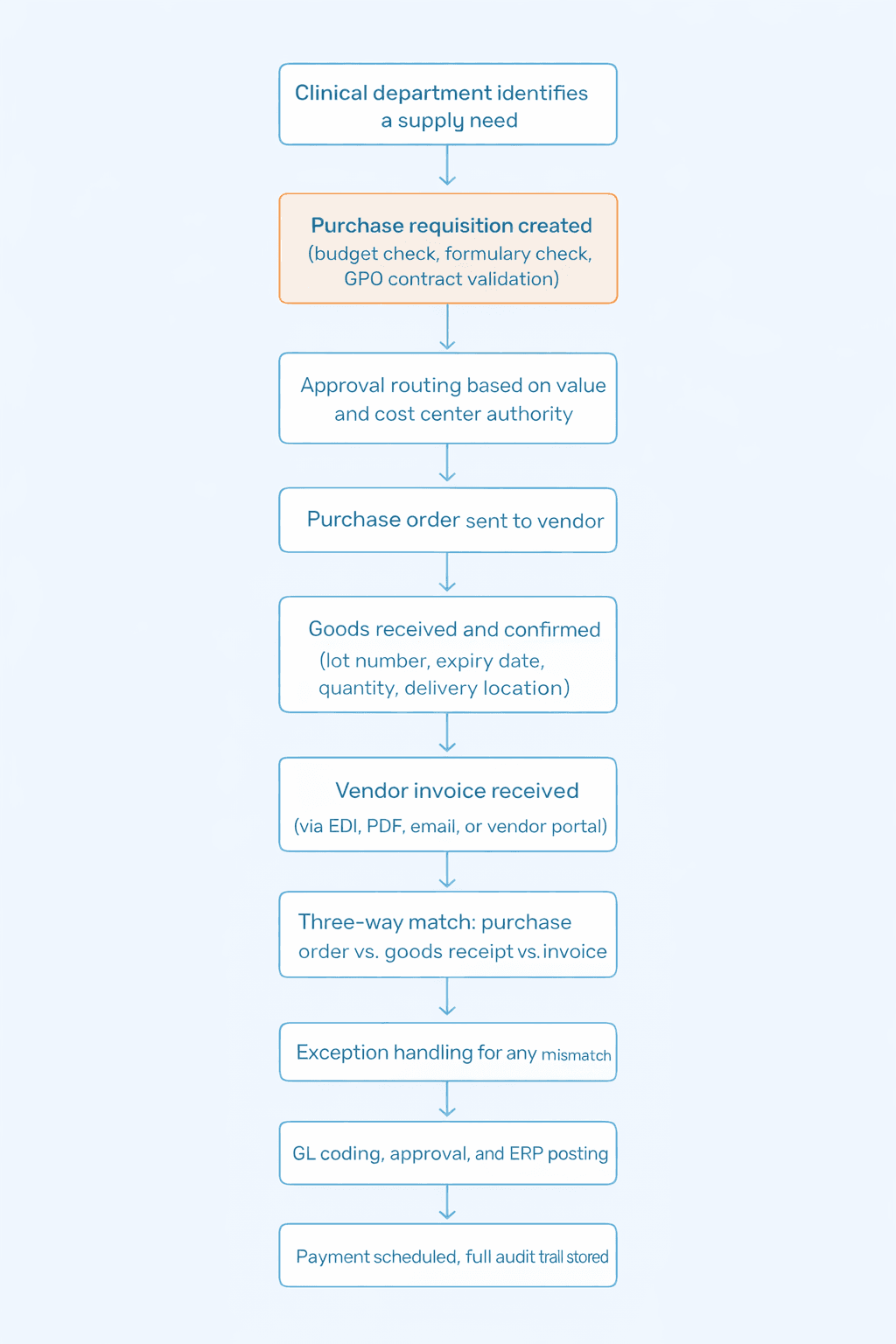
Every step is a place where things can slow down or require manual intervention. In a hospital processing thousands of invoices a month, the cumulative cost of that friction is significant.
The Four Things Healthcare ERPs Get Wrong, Even the Good Ones
Invoice matching for medical supplies. A pharmaceutical invoice may need to match by lot number, expiry date, contracted unit price, and GPO compliance, all at once. Systems that handle standard matching often treat this as an exception and route it to a human. When you have hundreds of these daily, that is a staffing problem.
Multi-entity management. A regional health system might include a hospital, clinics, a physician group, and a foundation, each with its own budget authority. Many ERPs require significant customization to enforce entity-level controls and consolidate accurately, and customization adds cost and complexity.
Fund and grant accounting. Most US hospitals are not-for-profits. Grant funds from federal agencies and private donors come with strict rules about how money can be spent. Systems that treat this as an add-on rather than a core capability create significant extra work at audit time.
Access controls beyond standard software. Healthcare finance documents touch patient-adjacent information: invoices reference clinical departments, budgets reflect patient volumes. Standard ERPs log transactions. Healthcare finance also needs logs of who accessed which records and when.
Where Every Healthcare ERP Hits a Wall
An ERP is a system of record. It stores and reports on transactions. It is not designed to automatically process high volumes of incoming invoices. That gap is where AP teams spend most of their time.
Invoices arrive from different vendors in different formats: EDI from one distributor, a PDF from a contractor, a Word document from a professional services firm. Each has to be read, matched, coded, routed for approval, and posted. Multiply this across hundreds of vendors and thousands of transactions a month, and the scale becomes clear.
Most ERPs handle posting and recording well. The reading, matching, and routing is largely left to the AP team to do by hand. This is why healthcare finance teams are large relative to the organizations they support.
How the Main ERP Platforms Compare for Healthcare
Want to understand how the major ERP vendors stack up in the market, which platforms are gaining share in healthcare, and what the shift toward industry-specific tools means for your buying decision? Our guide to ERP systems market share in 2026 covers the full picture, from vendor trajectories to what buyers are prioritizing right now.
Platform | Best Suited For | Strengths | Where It Falls Short |
Oracle NetSuite | Mid-sized health systems, ambulatory networks | Strong multi-entity management, true cloud | Healthcare-specific matching needs configuration |
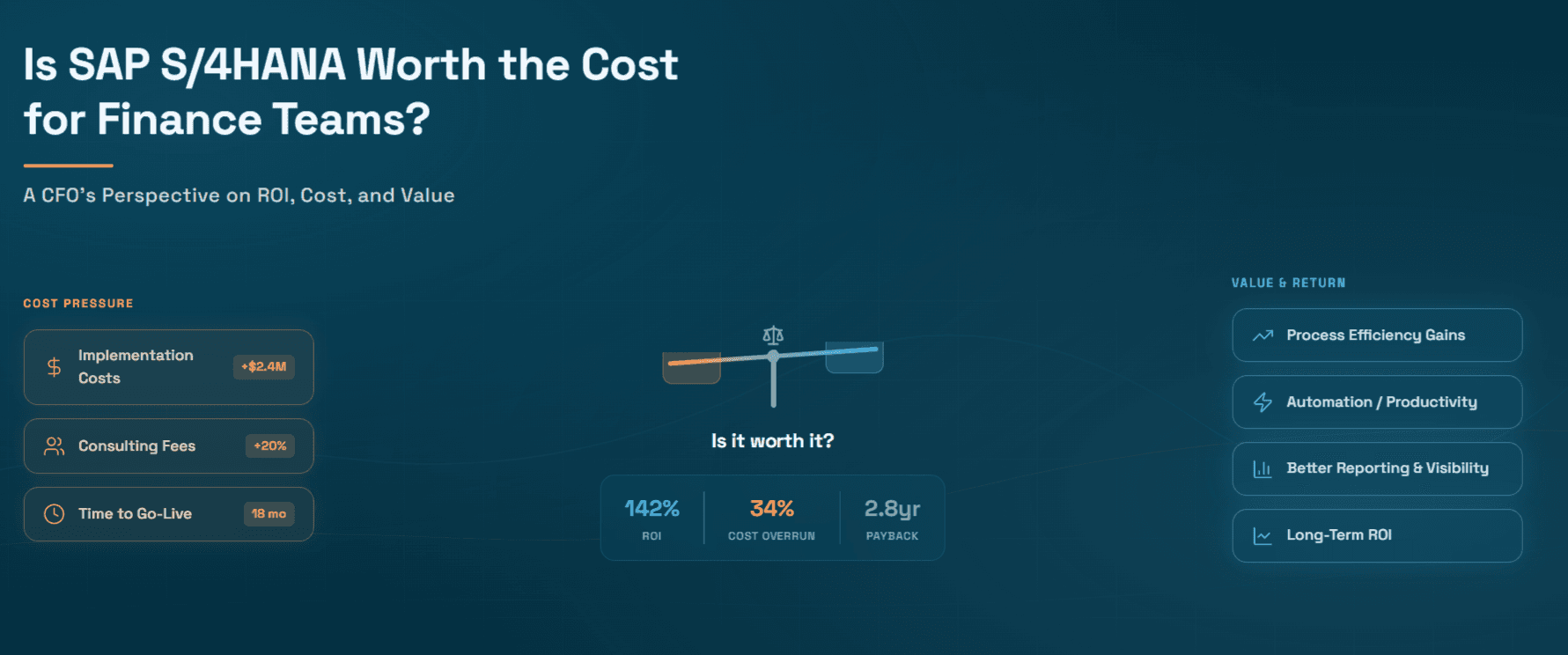
SAP S/4HANA | Large academic medical centers, complex systems | Deep configurability, sophisticated procurement | Long, expensive implementation, steep learning curve |
Microsoft Dynamics 365 BC | Physician groups, smaller clinics | Familiar for Microsoft users, clean interface | Limited fund accounting without add-ons |
Sage Intacct | Not-for-profit health systems, community health | Fund accounting built into core design | Less suited for large acute care complexity |
The honest truth: the platform choice matters less than most evaluation processes suggest. What matters more is what you build on top of it.
What AI Automation Does That the ERP Cannot
After the ERP goes live, the AP team is still receiving invoices in a dozen formats, manually keying data, resolving matching exceptions, and chasing approvals. The volume does not decrease because you changed platforms.
AI automation tools sit on top of the ERP and handle the work its native modules leave to humans: reading invoices, extracting data, running matches, flagging exceptions with context already attached, and feeding everything back into the ERP automatically.
For procurement, automated purchase orders eliminate manual steps between a requisition and a dispatched PO. Budget checks run against live ERP data before the order is placed, not after the invoice arrives.
For compliance, a structured approach to vendor management ensures insurance certificates and exclusion list screenings are tracked and flagged before they become audit findings.
The ERP remains the system of record. The automation layer handles the volume and complexity the ERP was never designed to absorb alone.
How Hyperbots Specifically Helps Healthcare Finance Teams
Most ERP gaps in healthcare come down to one problem: the ERP was not designed for the intersection of clinical operations, supplier complexity, and multi-payer revenue. Hyperbots is built precisely for that intersection.
It connects directly to the ERPs healthcare organizations already run, including Oracle NetSuite, SAP S/4HANA, SAP ECC, SAP B1, Microsoft Business Central, Sage Intacct, and Sage 300, through pre-built native connectors. No custom integration to build or maintain.
Invoice Processing. The Invoice Processing Co-Pilot validates supplier invoices using patient, procedure, and case-level clinical context before posting to the ERP. For healthcare teams dealing with the complexity of three-way matching across pharmaceutical lot numbers, contracted prices, and GPO compliance, this is where most manual effort is eliminated. Result: 99.8% extraction accuracy, 80% straight-through processing, 80% reduction in invoice processing costs.
Procurement. The Procurement Co-Pilot guides purchase requests toward approved vendors and contract-compliant items, controlling the off-contract spend that clinician preferences drive. Purchase requisitions are created in under 5 minutes. PO creation and dispatch time is reduced by 80%.
Accruals. Hyperbots continuously estimates accruals by reading open POs, partial goods receipts, and vendor billing patterns. Variance between accrued and actual costs stays below 5%.
Payments. Hyperbots automates clinician-dependent approval workflows and optimizes payment timing to capture early payment discounts while protecting critical supplier relationships.
Collections. DSO is reduced by 40%, unapplied cash drops by 90%, and collections costs fall by 70%. Cash flow improves by 10%.
Cash Application. ERA (835) and EOB data is processed automatically. Partial and short payments are resolved without manual matching, reducing unapplied cash by 90%.
Vendor Management. The Vendor Management Co-Pilot keeps credentials verified, flags expired documentation proactively, and prevents non-compliant vendors from entering the payment cycle.
Sales Tax Verification. Tax treatment varies across medical products, devices, and services. Hyperbots validates charges on every invoice and generates audit-ready documentation automatically.
Healthcare organizations go live within one month. ROI is typically reached within six months.
Area | The Problem | What Hyperbots Delivers |
Invoice Processing | Diverse formats, clinical mismatches | 99.8% accuracy, 80% STP, 80% cost reduction |
Procurement | Off-contract spend, slow PO cycles | 5-min PR creation, 80% faster PO dispatch |
Accruals | Manual estimation, high variance | Less than 5% variance, accrued vs actual |
Payments | Delayed approvals, supply risk | Automated routing, optimized timing |
Collections | Fragmented multi-payer follow-up | 40% DSO reduction, 70% cost reduction |
Cash Application | Unapplied cash, batch-to-claim matching | 90% unapplied cash reduction |
Vendor Management | Expired credentials, compliance gaps | Proactive flagging, audit-ready records |
Sales Tax | Incorrect tax on medical invoices | Verified charges, audit-ready documentation |
Reconciliations | Manual cross-system matching | 80% reduction in reconciliation cost |
Go-Live | Long, disruptive implementations | Live within one month |
The Audit Question That Reveals Everything
Here is a simple test. If an auditor arrived today and asked for line-item documentation on 200 vendor invoices from the past 18 months, how long would it take to produce them?
If the answer is hours, your system is working. If the answer is days, or if it involves reconstructing records from memory and bank statements, the ERP and the processes on top of it are not doing what they need to do.
The right combination of ERP and automation makes that request a filtered export, not a search party. That is the standard healthcare finance should be held to, and it is achievable.